Cardiac Troponins for the Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease
Clinical question: Does using dynamic changes in high-sensitivity troponin I (hsTnI) and T (hsTnT) outperform using standard static cutoffs for diagnosing non-ST elevation myocardial infarction (NSTEMI) in chronic kidney disease (CKD) patients?
What was already known: Patients with chronic kidney disease (CKD) are at high risk for myocardial infarction (MI), but cTnI and cTnT are often nonspecifically elevated in CKD patients, posing a challenge to diagnosing CKD patients presenting with suspected MI.
Methods: This study included 8553 patients, including controls and CKD patients. 1494 patients comprised the retrospective cohort, and data was extracted from a clinical registry (hsTnI was used). 7059 comprised the prospective cohort, for which hsTnT was collected at 0 and 3 hours after presentation. Patients on dialysis or with anemia (Hgb <10) were excluded)
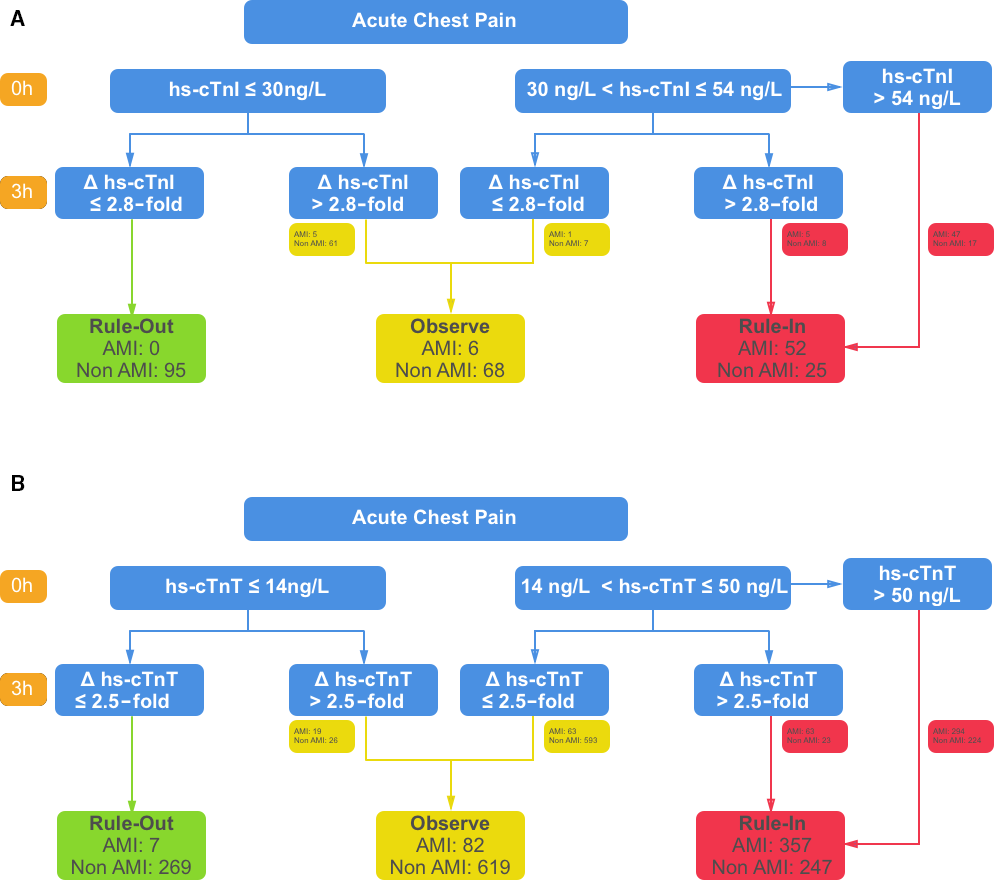
Results/implications: Static cutoffs for hsTnI and hsTnT have low specificity in detecting NSTEMI in CKD patients, in whom troponin can be chronically elevated even without acute injury. Increasing the static cutoff for CKD patients comes with the cost of decreased sensitivity. The authors propose optimized dynamic cutoffs that utilize serial troponin measurements for CKD patients (outlined in the figure) that have a higher diagnostic accuracy (69% for hsTnI and 55% for hsTnT) than traditionally used static cutoffs.
Bottom line: In patients with CKD and suspected NSTEMI, using serial troponin measurements and the suggested optimized cutoffs rather than static HST cutoffs yields higher diagnostic accuracy.